How is the slave trade linked to the spread of HIV in Africa?

Stay up to date:
Future of Global Health and Healthcare
A recent law that legalised polygyny1 in Kenya caused a stir not only in Kenya’s parliament and among women’s rights groups, but also among HIV/AIDS activists – the perception being that the likelihood of infidelity is higher in polygynous marriages (Kwena et al. 2014). Since sexual habits involving multiple partners are recognised as one of the main channels of transmission of HIV (Halperin and Epstein 2004), extramarital partnerships are thought to lead to higher HIV infection rates.
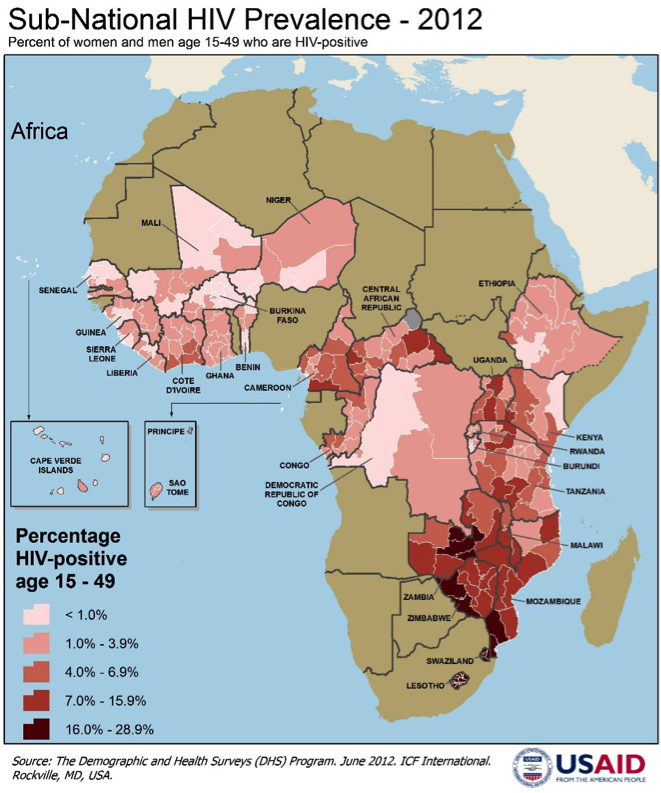
HIV/AIDS is one of the most deadly diseases in Africa. According to the World Health Organization (2012), 1.6 million people died of AIDS around the world in 2012, and 75% of them were in sub-Saharan Africa. Figure 1 shows the geographical distribution of HIV prevalence at the sub-national level for the 15-49 year-old age group in the countries covered by the Demographic and Health Survey Program.
Figure 1 Sub-national HIV prevalence, 2012
What is peculiar about sub-Saharan Africa is also that HIV is much more common among women, who represent 75% of the infected in the 17-24 year-old age group (UNAIDS 2013). Harmful gender norms, inequalities between the sexes, and women’s rights violations are among the reasons why women are believed to be more vulnerable to the virus. How can polygyny contribute to this pattern?
The slave trade and polygyny
Previous research found that the diffusion of polygyny in Africa was reinforced by the transatlantic slave trade, which for over almost four centuries took away more men than women and thus lead to distorted sex ratios (Edlund and Ku 2011, Dalton and Leung 2014, Fenske 2015).
The link between polygyny, the spread of the HIV epidemic, and its gendered pattern is the subject of our new research (Bertocchi and Dimico 2015) based on the hypothesis that the slave trade and the consequent demographic shock may at the same time have encouraged polygyny and high-risk sexual behaviour. Indeed, in a polygynous family men have sexual relationships with multiple women, while at the same time unsatisfied co-wives are more likely to engage in extramarital partnerships. Co-habitation of co-wives can then multiply the speed of transmission among women.
The role of the demographic shock following the slave trade as a sort of primordial risk factor for the spread of HIV is tested using clustered-level data on HIV infection rates, polygyny and sexual behaviour provided by the Demographic and Health Survey. Information on HIV infection is collected by the Demographic and Health Survey on the basis of a blood test. The survey also collects information on the number of co-wives, the intensity of sexual activity and the frequency of extramarital partnerships.
Historical, spatially disaggregated data on population growth in Africa is obtained from the History Database of the Global Environment. In Figure 2, a map showing population growth over the period 1500-1860 is overlaid with Demographic and Health Survey clusters. The darker the area of the map, the lower the rate of population growth experienced over the time period (note that white areas represent missing values). The map suggests that during the slave trade period the negative demographic shock was more severe in West Africa. Indeed, by combining the population growth data with the transatlantic slave trade data from Nunn and Wantchekon (2011), the negative influence of the latter on population growth over the period running from 1500 to 1860 is confirmed.
Figure 2. African Population Growth in 1500-1860

Source: Bertocchi and Dimico 2015.
The demographic shock turns out to have influenced the contemporaneous incidence of polygyny, since in areas affected by slower population growth in 1500-1860, men are currently more likely to have more than one wife. Table 1 presents a cross-tabulation showing that polygyny today is less widespread in clusters that exhibited faster population growth over the relevant period.2
Table 1. The demographic shock and polygyny
Population growth in 1500-1860 Polgyny Mean Stand. Dev. Freq. 0 .232 .253 162,222 1 .202 .225 41,705 Total .229 .248 203,927Polygyny, risky sexual behaviour, and HIV infection
The demographic shock is also found to be associated with contemporaneous sexual habits and along gender-specific patterns. In clusters affected by a larger demographic shock, men (but not women) display more intense sexual activity and women (but not men) are more likely to engage in extramarital partnerships. The latter finding is illustrated in Table 2, where female infidelity today is shown to be less widespread in clusters that historically exhibited faster population growth. Combined with previous evidence on the prevalence of polygyny, these outcomes are consistent with the hypothesis that neglected co-wives are more likely to be unfaithful.
Table 2. The demographic shock and female infidelity
Population growth in 1500-1860 Femal infidelity Mean Stand. Dev. Freq. 0 .211 .248 283,427 1 .178 .250 43,056 Total .206 .248 326,483The above preliminary findings are crucial to assess the link between polygyny and HIV infection, which may be plagued by reverse causality. Using the demographic shock as an instrument for polygyny, it is indeed established that in clusters where polygyny is more widespread, HIV infection rates are higher. Turning to the channels of transmission – the risky sexual habits induced by polygyny – reverse causality emerges as a critical issue since risky sexual behaviour favours HIV infection and, in turn, infected people are likely to modify their behaviour. Again this endogeneity issue can be addressed by employing the demographic shock as an instrument. Results show that clusters exhibiting more frequent female extramarital partnerships are affected by significantly higher infection rates.
Conclusion
The demographic shock induced by the slave trade represents a primordial risk factor that is still shaping contemporary family structures and sexual behaviour. The empirical evidence is consistent with the hypothesis that polygyny is associated with unsatisfying marital relationships, particularly for women, with consequent marital infidelity and an increased risk of infection, which is in turn magnified for women cohabiting within polygynous households.
In light of these findings, policymakers and human rights organisations should understand that the struggle against HIV/AIDS involves the eradication of deeply rooted beliefs and practices that date as far back as to the pre-colonial history of the African continent.
References
Bertocchi, G and A Dimico (2015), “The Long-Term Determinants of Female HIV Infection in Africa: The Slave Trade, Polygyny, and Sexual Behavior”, CEPR Discussion Paper No. 10654.
Dalton, J T and T C Leung (2014), “Why Is Polygyny More Prevalent in Western Africa? An African Slave Trade Perspective”, Economic Development and Cultural Change 62: 599-632.
Edlund, E and H Ku (2011), “The African Slave Trade and the Curious Case of General Polygyny”, MPRA Paper No. 52735.
Fenske, J (2015), “African Polygamy: Past and Present”, Journal of Development Economics, forthcoming.
Halperin, D T and H Epstein (2004), “Concurrent Sexual Partnerships Help to Explain Africa’s High HIV Prevalence: Implications for Prevention”, Lancet 364: 4-6.
Kwena, Z, I Mwanzo, C Shisanya, C Camlin, J Turan, L Achiro and E Bukusi (2014), “Predictors of Extra-Marital Partnerships among Women Married to Fishermen along Lake Victoria in Kisumu County, Kenya”, PLoS ONE 9, e95298.
Nunn, N and L Wantchekon (2011), “The Slave Trade and the Origins of Mistrust in Africa”, American Economic Review 101: 3221-3252.
UNAIDS (2013), “Global Report: UNAIDS Report on the Global AIDS Epidemic”, UNAIDS, Geneva.
World Health Organization (2012), “World Health Statistics 2012”, World Health Organization, France.
Endnotes
1 Polygyny is the instance of a man having more than one wife at the same time. Polygamy is the general custom or practice of having more than one wife.
2 Two-stage least-squares estimates establish that the observed link is indeed causal.
This article is published in collaboration with VoxEU. Publication does not imply endorsement of views by the World Economic Forum.
To keep up with the Agenda subscribe to our weekly newsletter.
Author: Graziella Bertocchi is Professor of Economics at the University of Modena and Reggio Emilia, Italy. Arcangelo Dimico is a Lecturer in Economics at the Queen’s University of Belfast.
Image: Pharmaceutical tablets and capsules in foil strips are arranged on a table in this picture illustration taken in Ljubljana September 18, 2013. REUTERS/Srdjan Zivulovic
Don't miss any update on this topic
Create a free account and access your personalized content collection with our latest publications and analyses.
License and Republishing
World Economic Forum articles may be republished in accordance with the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International Public License, and in accordance with our Terms of Use.
The views expressed in this article are those of the author alone and not the World Economic Forum.
Forum Stories newsletter
Bringing you weekly curated insights and analysis on the global issues that matter.
More on Geographies in DepthSee all

Kaiser Kuo
June 24, 2025

Kaiser Kuo
June 19, 2025

Aimée Dushime
April 18, 2025

Samir Saran and Anirban Sarma
April 17, 2025

Nada AlSaeed
April 16, 2025

Zhang Xun and Vee Li
April 8, 2025